
Key points:
- Pain radiating into the buttock, thigh, leg, and foot = sciatica
- Paralysis, sphincter disorders = emergency consultation
- 80% of cases resolved without surgery within 6 weeks
Diagnosis
Consult your primary care physician, who will review your medical history, symptoms, and perform a clinical examination. They may prescribe one or more of the following tests:
-
MRI
Test of choice — much more precise than a CT scan. The MRI detects which disc is damaged, if there is nerve compression, or another diagnosis (spinal stenosis, spondylolisthesis, tumor, etc.).
-
CT Scan
Complementary to MRI: it precisely visualizes the bone of the vertebrae, useful in treatment strategy.
-
Electromyogram (EMG)
Helps identify which nerve is affected in case of clinical or radiological doubt. It measures nerve conduction velocity via small needles placed in the muscles.
Treatments
Conservative treatment is always the first step. With a well-managed approach, 80% of patients experience a reduction or disappearance of pain within approximately 6 weeks. Surgery is only considered in cases of failure or severe symptoms.
Non-surgical treatments
- Self-care and relative rest In most cases, pain subsides within a few days and disappears within 4 to 6 weeks with a slight reduction in activity.
- Medications Anti-inflammatories (NSAIDs), analgesics, muscle relaxants, short-term oral corticosteroids. Corticosteroids can provide rapid relief (24h) but have side effects with prolonged use.
- Epidural corticosteroid injections Performed under radiological guidance. Approximately 50% of patients experience relief — results are often temporary, lasting from weeks to several years.
- Physiotherapy Strengthening of back, leg, and abdominal muscles. Work on posture, stretching, and flexibility. Strengthening exercises are a key element to continue throughout life.
- Complementary therapies Some patients find acupuncture, meditation, or biofeedback useful in pain management.
Surgical Treatments
Considered in cases of failed conservative treatment, intolerable pain resistant to analgesics, or signs of nerve damage (weakness, loss of sensation). In cases of paralysis or sphincter disorders, emergency intervention may be necessary.
- Microsurgical discectomy Small incision in the back, muscle retraction, resection of the ligamentum flavum and part of the bone to expose the nerve root. The disc fragment compressing the nerve is removed under a microscope. Approximately 90% of patients recover well and resume activity within 6 weeks.
- Minimally invasive microendoscopic discectomy Even smaller incision, with progressive dilators creating a tunnel to the vertebra. Less muscle damage, faster recovery. Not applicable to all herniated discs.
Post-operative Period
Relief is most often immediate. Convalescence is approximately 4 to 6 weeks with a gradual resumption of activities. Physiotherapy is often recommended. Return to sports occurs after the convalescence period; a gradual return to work (part-time therapeutic) is sometimes necessary depending on the professional activity.
The symptoms of a herniated disc vary considerably depending on the location of the herniation and your own reaction to the pain. If you have a herniated lumbar disc, you may feel pain radiating from your lower back, down one or both legs and sometimes to your feet (called sciatica). You may feel pain similar to an electric shock.
Activities such as bending, lifting, twisting and sitting can trigger or increase pain. Lying flat on your back with knees bent, or on your side in a "dog-leg" position, can provide relief, as it reduces the pressure exerted on the disc.
Sometimes the pain is accompanied bynumbness and tingling in the leg or foot. It can also be associated with cramps or muscle spasms in the back or leg.
In addition to pain, you may experience muscle weakness in the leg, with a reduction or loss of reflexes in the knee or Achilles tendon. In the case of paralysis, the foot may fall when walking and the toe rubs on the ground. The knee may give way when walking and the leg may give way, leading to a fall. This means that the muscles of the thigh or leg are paralyzed. Likewise, the bladder can become paralyzed, with urine retention followed by urine loss. These are signs of seriousness. If you experience leg weakness or bladder control difficulties, you should seek immediate advice from a neurosurgical department.
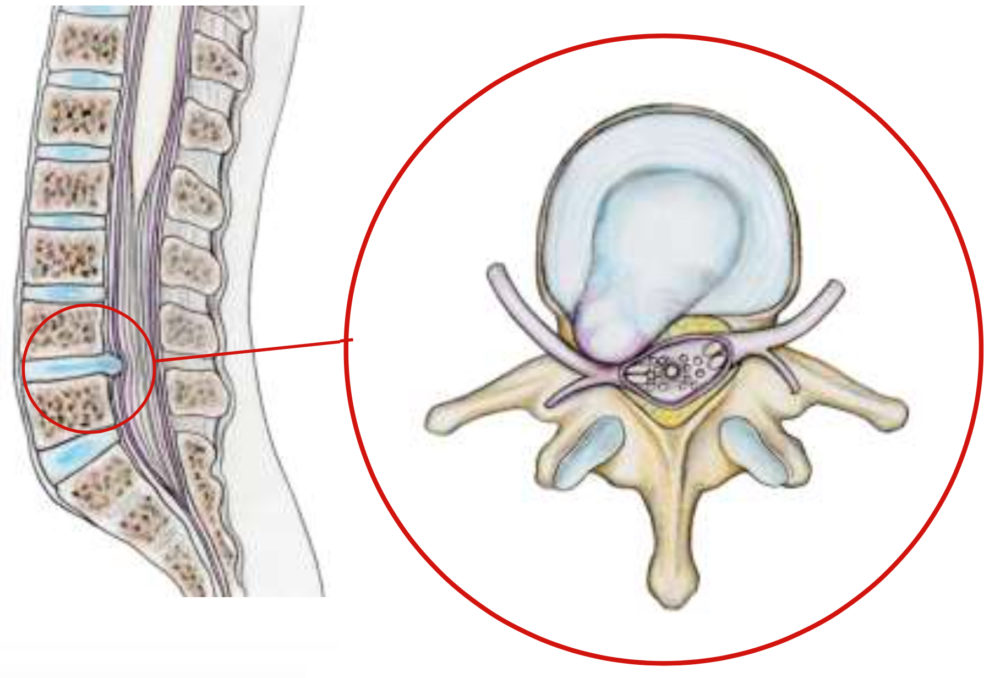
The hernia may migrate backwards in the event of a false move : lifting effort, moving house, violent sporting gestures..... It can also occur spontaneously without any triggering factor. Aging plays an important role. With age, discs dry out and become progressively softer and more pasty. The fibrous outer wall of the disc may weaken, allowing the herniation to migrate. Migration of the herniated disc through the posterior part of the annulus is the cause of back pain, which can be extreme: lumbago with a sensation of "blockage". Compression of the nerve by the hernia causes pain in the leg.
Genetics, smoking and a number of occupational and recreational activities can lead to early degeneration of the disc.
A herniated disc can affect many people, but it most often occurs in adults between 30 and 60 years old. It corresponds to the displacement of a part of the intervertebral disc, located between two vertebrae, which can compress a nerve and cause pain.
People at Higher Risk
Certain situations or characteristics increase the risk of developing a herniated disc:
1. Age
Over time, intervertebral discs gradually lose their elasticity and shock-absorbing capacity. This natural aging phenomenon can promote the appearance of a herniation.
2. Intense or Repetitive Physical Activities
Occupations or activities involving heavy lifting, repetitive back movements, or strenuous postures (manual handling, construction, care, logistics) can place significant stress on the spine.
3. Sedentary Lifestyle and Lack of Muscle Strengthening
A lack of physical activity can weaken the muscles that support the spine, particularly the back and abdominal core muscles.
4. Certain Sports or Sudden Efforts
A twisting motion, intense effort, or a wrong movement can sometimes trigger symptoms in a person whose disc is already weakened.
5. Individual Factors
Overweight, smoking, or certain genetic predispositions can also contribute to the wear and tear of intervertebral discs.
Lumbar and Cervical Herniated Disc
A herniated disc can occur at different levels of the spine:
In the lumbar region (lower back): this is the most common form. It can cause sciatica or cruralgia.
In the cervical region (neck): rarer, it can lead to arm pain, sometimes called cervicobrachial neuralgia.
A Common but Often Benign Condition
A herniated disc is a common pathology. In the majority of cases, symptoms improve with medical treatment and appropriate rest.
Surgery is only considered in certain specific situations, particularly when pain persists despite treatments or when there are neurological signs.