Who's affected?
A very rare tumor, accounting for 6% of skull base tumors. Patients are most often between 30 and 50 years old, both women and men. In the vast majority of cases, chondrosarcomas are isolated but can occur in the context of diseases such as Ollier's disease or Paget's disease.
Symptoms
The tumor develops slowly, with symptoms generally appearing late. At the skull base, the most frequent symptoms are headaches and double vision. Others may occur: visual or hearing loss, difficulty swallowing, hoarse voice, gait disturbances, motor weakness.
Diagnosis
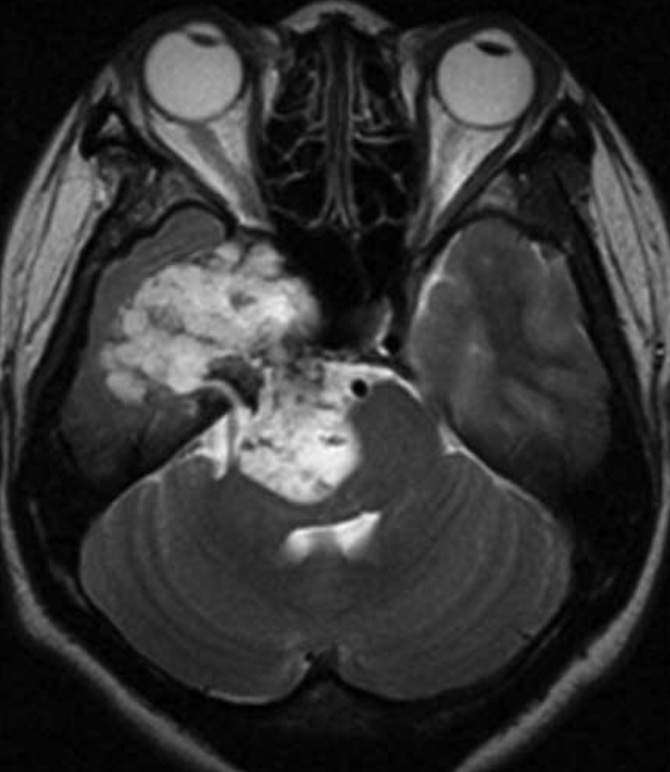
CT scans and especially MRI allow for a strong suspicion of the diagnosis thanks to the characteristic appearance and typical location of these tumors. As it is a rare tumor, diagnosis requires experienced radiologists — the distinction between chondrosarcoma and chordoma can be difficult on imaging. The definitive diagnosis is established by anatomopathological analysis after excision.
Types of Chondrosarcomas
Several types are distinguished, including conventional forms (the most frequent), clear cell, mesenchymal, and dedifferentiated. Clear cell and dedifferentiated forms are exceptional at the skull base. Mesenchymal forms are rarer and more aggressive, with a high risk of recurrence.
Conventional Chondrosarcomas
Subdivided into grades I, II, and III. Grades I and II are the most common. The risk of recurrence increases with grade.Rare Forms
Clear cell, mesenchymal (more aggressive), and dedifferentiated chondrosarcomas — exceptional at the skull base.Treatment
Multidisciplinary approach
A multidisciplinary approach is crucial. A monthly national multidisciplinary team meeting (MDT) brings together all involved stakeholders. We collaborate with:
- ENT Department and Neuroradiology Department of Lariboisière Hospital
- Orsay Proton Therapy Department — Institut Curie (Dr. Hamid Mammar, Dr. Valentin Calugaru)
- Institut Gustave Roussy (Dr. Stéphanie Bolle)
- Biopsy Rarely necessary. However, it can be useful when the distinction between chondrosarcoma and chordoma is difficult, in order to adapt the surgical strategy.
- Surgery Must be performed in experienced centers for skull base neurosurgery. The objective is to remove as much of the tumor as possible while preserving critical nervous and vascular structures in the immediate vicinity. Excision also prepares the ground for complementary radiotherapy.
- Proton Therapy / Radiotherapy The 5-year recurrence risk is approximately 30 to 40%. Depending on the degree of resection and tumor grade, high-dose radiotherapy is indicated. The reference technique is proton therapy (Orsay center) — Dr. Mammar, Dr. Calugaru, Dr. Bolle. Hypofractionated stereotactic radiosurgery may be offered for small volume residuals or localized recurrences.
- Chemotherapy Reserved for aggressive and recurrent forms that cannot be reoperated. These situations remain relatively rare at the skull base.