Diagnosis
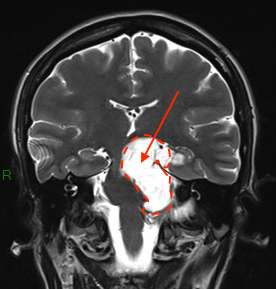
On CT scan, the epidermoid cyst appears as an iso- or hypodense mass, heterogeneous, with irregular contours, without contrast enhancement or perilesional edema.
The diagnosis is confirmed by MRI, and particularly by hyperintensity on diffusion-weighted sequences—sequences that are essential for confirming the diagnosis with certainty.
Treatment
With very slow progression, they are most often monitored with regular MRI scans. Surgery is recommended in case of symptoms. If symptoms are moderate and the operative risk is significant, surveillance may be preferred initially.
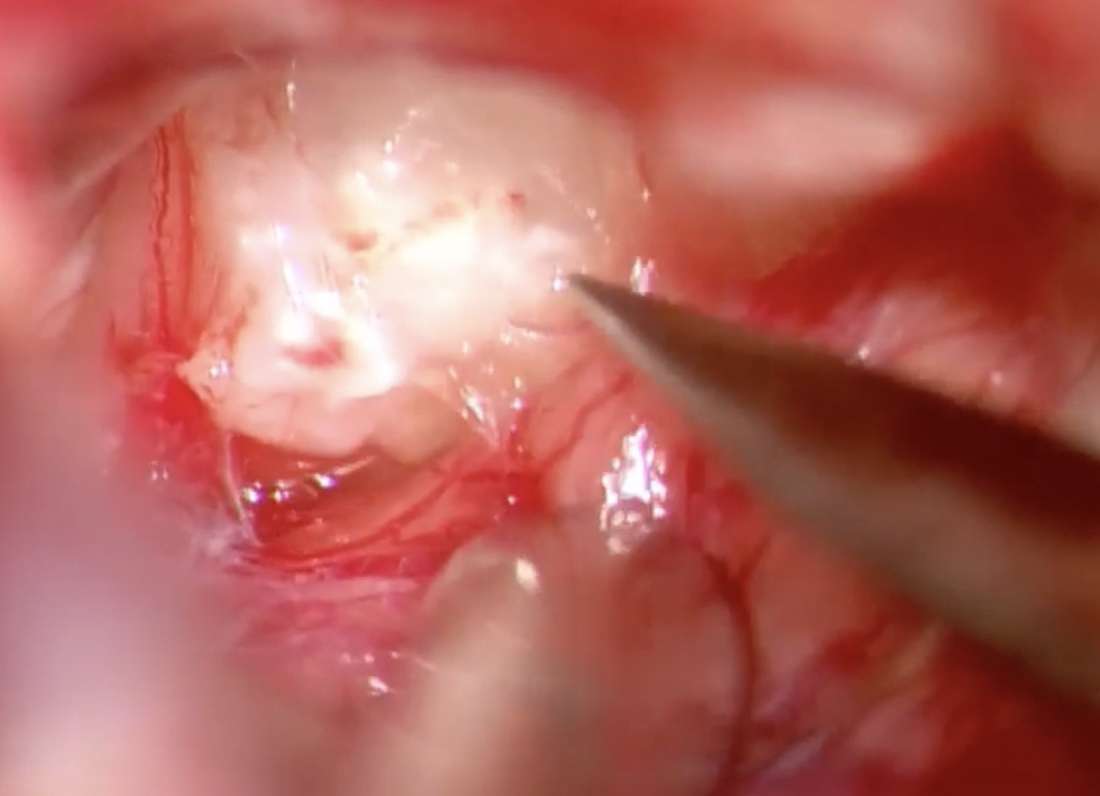
- Complete resection—primary objective The treatment of choice is total resection of the tumor, including the capsule. Since the capsule produces the cystic content, leaving it in place carries a high risk of recurrence. Complete resection is particularly important during the first intervention, as postoperative scarring makes any subsequent surgery even more difficult.
- Partial resection Sometimes unavoidable when the cyst is in close proximity to critical neural or vascular structures. Part of the capsule is then left in place, with a significant risk of long-term recurrence.
- Surgical approach It depends on the location of the cyst. Some large cysts require complex skull base approaches to allow complete removal while preserving neural and vascular structures.
Course and prognosis
Progression is very slow. After surgery, if part of the capsule is left in place, the risk of recurrence is significant—often after many years. Reoperation is sometimes necessary.
The overall prognosis is favorable, but these cysts often require complex intervention that is not without risks, requiring specific surgical expertise. Malignant transformation is exceptional.
They are most often located deep beneath the brain or in front of the brainstem and cerebellum, making them difficult to remove. They are considered to be injuries to the base of the skull.
The most common locations are :
- the cerebellopontine angle
- suprasellar regions
- the sylvan valley
- the ventricular system, in particular the 4th ventricle,
- the pineal region
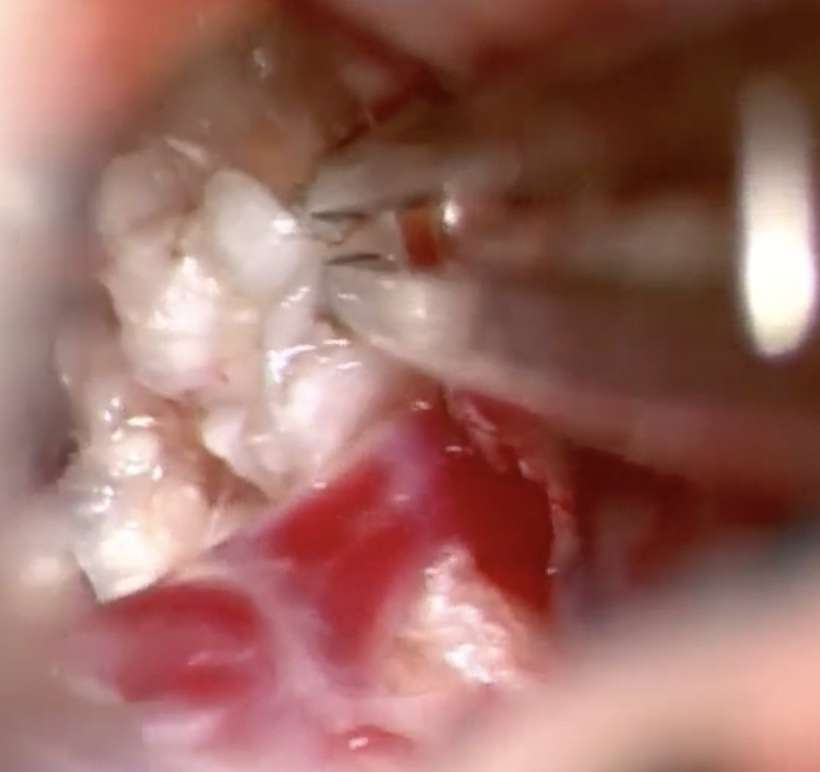
Epidermoid cysts are also known as "pearly" tumors, due to their pearly-white color and nippled appearance.
Histologically, they consist of a stratified, keratinized epithelial wall delimiting a cavity in which the degradation products of desquamated epithelial cells accumulate in the form of an amorphous material rich in keratin and cholesterol.
The rarer dermoid cyst does not usually have the milky-white appearance so characteristic of its epidermoid counterpart. It is more variable, more heterogeneous, due to the diversity of materials that collect in its cavity. The epithelial lining is identical, but its wall also contains dermal elements: hair follicles, sebaceous and sweat glands, and sometimes even fat lobules. The cystic content is thus a more or less heterogeneous amalgam of keratin, cholesterol, sebaceous and sweat secretions, giving a more yellowish appearance, often with hairs.
Their growth is very slow and symptoms occur late.
Symptoms vary depending on tumor location:
– headaches, although it is often difficult to determine whether the headaches are related to the lesion or not,
– dizziness,
– balance disorders,
– involvement of one or more cranial nerves: facial pain, double vision, hearing loss, facial paralysis, hemifacial spasm, vision loss, visual field defect due to direct tumor compression of the nerves.
– epileptic seizures