 English
English
 Français
Français
{kind=link}
What is a cerebral arteriovenous malformation?
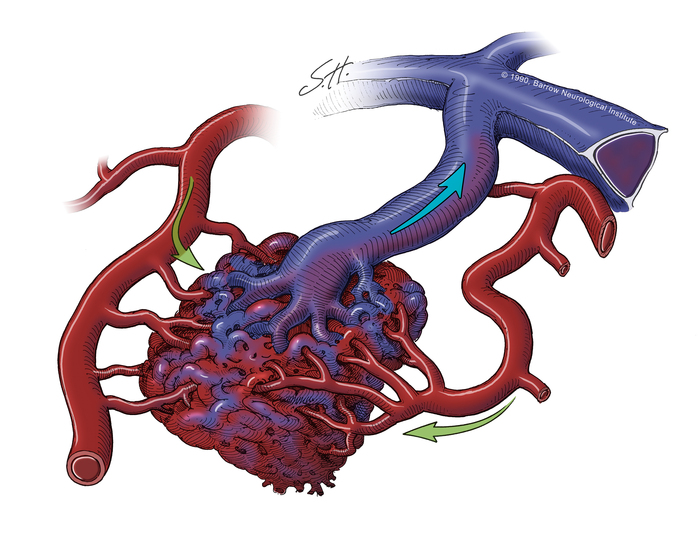
A cerebral arteriovenous malformation causes blood to flow directly from arteries to veins through a direct passway called a fistula instead of through capillaries forming what is called a “nidus”, in which the pressure is abnormally high leading to a risk of bleeding by rupture of the vascular wall estimated between 1 and 5 %/year. It can occur anywhere in the central nervous system. These may be more or less large malformations associated with variable venous drainage. Similarly, their location can be deep or more superficial in the brain and all of these criteria allow us to classify them and assess the treatment risk.
What is the presentation ?
These malformations are most often discovered when they are symptomatic but can also be discovered incidentally during a brain radiological examination (CT scanner or MRI) made for an unrelated disorder, because most people with AVMs experience few symptoms. The main presentation is a spontaneous cerebral hematoma. AVMs can also present with partial or generalized epileptic seizures in 30% of cases.
Symptoms may include :
- Headaches
- Nausea and vomiting
- Seizures
- Motor Weakness or paralysis
- Unbalance
- Tingling or numbness
- Dizziness
- Visual disturbances such as loss of part of the visual field
- Double vision
- Speech difficulties (aphasia)
- Memory loss
- Mental confusion
How is it diagnosed ?
Most arteriovenous malformations are detected through radiological examination, such as a CT or MRI scan.
Angiography, is used to confirm and study the malformation.
What are the treatment options ?
Depending on the clinical presentation, the AVM will be diagnosed urgently or in consultation and a decision will be proposed for its management, based on two options: Observation and radiological monitoring or specific treatment.
The latter is based on three modalities which are microsurgery, embolization and radiosurgery.
It is a multidisciplinary decision making process involving neurosurgeons and interventional neuroradiologists. A weekly multidisciplinary meeting is organized to discuss cases, but in the event of an emergency, the specialists meet consult each other urgently to define the best treatment strategy.
It is not uncommon for a multimodal treatment to be decided, combining an endovascular procedure and a surgical procedure, depending on the configuration of the malformation. Radiosurgery is best for post-therapeutic residues and small asymptomatic, epileptogenic or eloquent AVMs when other therapeutic modalities are considered too risky for the patient.