 English
English
 Français
Français
{kind=link}
What is a meningioma?
A meningioma is a tumor that develops from the meninges. The brain and spinal cord are surrounded by an envelope called the meninges. The outermost layer, thicker, is called the dura mater. A second, thin and transparent membrane called the arachnoid doubles the dura. Meningiomas originates from cells of the arachnoid. Between the arachnoid and the brain is the cerebro-spinal fluid (CSF).
Because meningiomas tend to grow inside the skull, they gradually compress the brain or spinal cord and nerves and can cause neurological disorders.
The majority of meningiomas are not cancerous but benign and slow growing. However, some may be more aggressive.
What are the symptoms?
Some people with meningiomas have no symptoms. The tumor can be discovered during a radiological examination (CT or MRI) done for another reason.
The symptoms usually appear gradually and vary according to the location of the meningioma and the nervous structures (Brain, cranial nerves…) that it compresses.
Meningiomas can lead to headaches, convulsions, weakness in the arm or leg, speech difficulty, decreased vision, abnormal sensations, personality changes, balance problems, vertigo, hearing loss, loss of smell …
Classification
Meningiomas are classified into several grades. The treatment varies according to the grade defined by the analysis of a sample obtained at the time of the surgical operation.
Grade I: Benign meningiomas. They are slow growing. If meningioma does not cause symptoms, it is often more reasonable to follow it with MRI or CT before considering treatment.
Grade II: Atypical meningiomas. They are more aggressive with a higher risk of recurrence once removed. Some grade II meningiomas require radiotherapy after surgery.
Grade III: Malignant meningiomas. They are the most aggressive but they represent less than 1% of meningiomas. It is a serious pathology and the surgery is almost always followed by radiotherapy. The risk of recurrence is high.
Location
Meningiomas are named according to their location (frontal meningioma, temporal meningioma, meningioma of the cavernous sinus …) and can cause very different symptoms depending on their location.
The meningiomas of the skull base, located under the brain are the most complicated to treat because of their deep location and the difficulty of accessing them. These meningiomas require the use of specific surgical techniques which are the specialty of our department.
What are the causes?
Meningiomas are more common in women than in men, and hormonal factors may promote the development and growth of meningiomas. Some hormonal treatments can promote the growth of meningiomas.
Some people also have a genetic predisposition to develop meningiomas and some diseases like neurofibromatosis are more likely to give meningiomas. They are sometimes multiple.
Patients who have had encephalic radiotherapy for other reasons, such as childhood, are also at increased risk of developing meningioma(s).
Who is concerned?
Meningiomas account for about 30% of all primary brain tumors. They occur most often between 40 and 60 years. They are rare in children.
How is the diagnosis made?
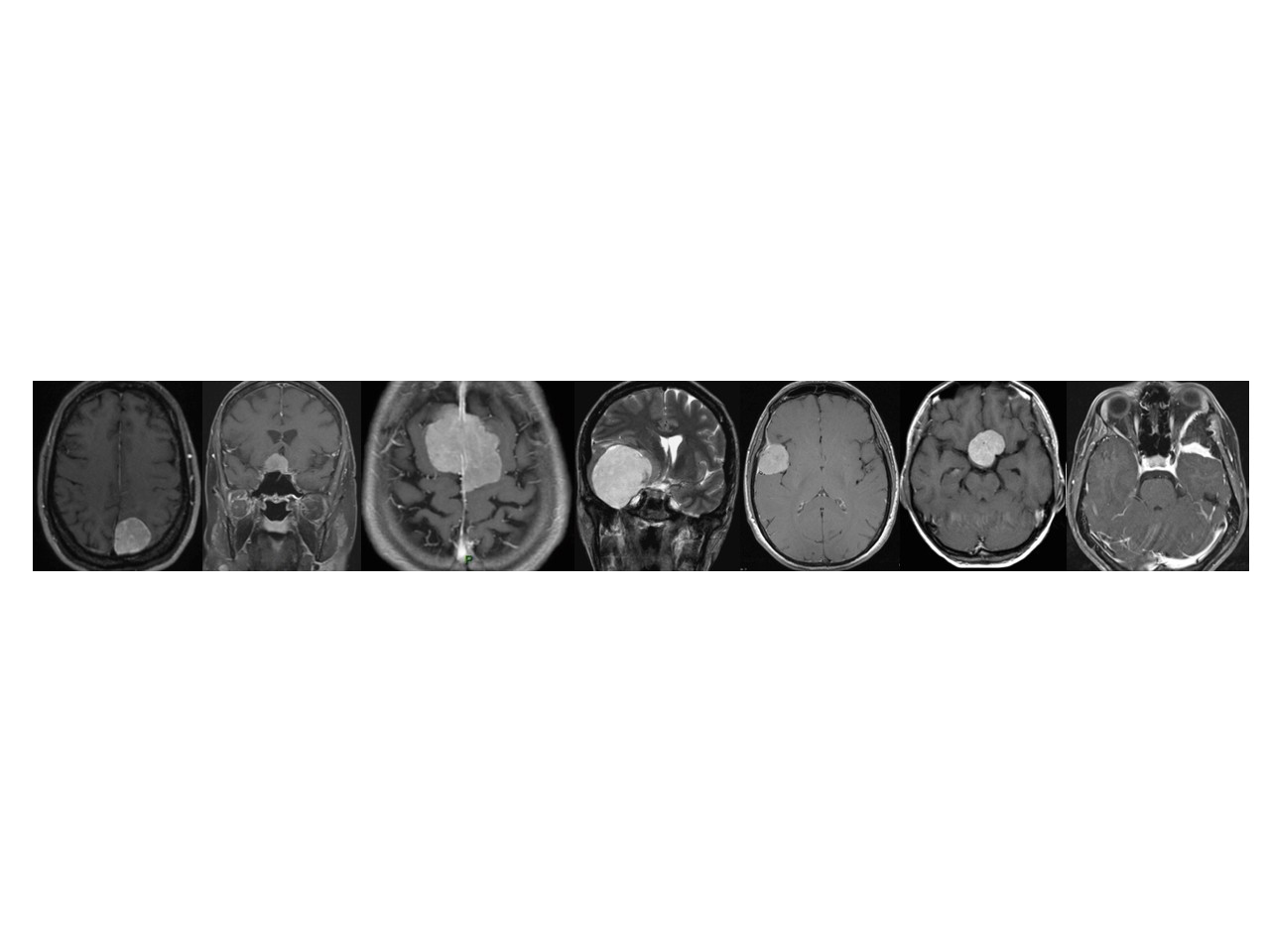
The lesion is discovered on CT (CT) or MRI (Magnetic Resonance Imaging), prescribed for symptoms suggestive of cerebral or medullary origin. Meningiomas being very characteristic, these examinations often make it possible to have a near certainty of the diagnosis.
What treatments are available?
Because they most often grow slowly, they do not necessarily have to be treated. Patient with few or no symptoms, can be followed with repeated MRI or CT scanner.
If they are to be treated, the options are surgery and radiation therapy. The proposed treatment will depend on the type, location and size of the meningioma, related disorders, age, health status.
Surgery
Surgical removal is the most common treatment for meningiomas that cause symptoms.
The risks of surgery vary according to the location of the tumor. To make the decision to operate, the risks of surgery should be considered lower than those related to the natural history of meningioma; It is therefore sometimes better to choose for a simple surveillance and let the meningioma evolve. Some surgeries are complex with significant risks when the meningioma is located in more threatening areas, deep as the base of the skull.
Advances in technology have improved the surgeon’s ability to precisely locate the tumor, define its boundaries, and avoid touching the functional and vital areas of the brain. They allow for safer and less invasive procedures.
These technological advances include neuronavigation, neuro-monitoring, endoscopy, ultrasound scalpels, micro-doppler …
Radiotherapy
Radiation therapy is indicated when the removal of the meningioma is incomplete and the tumor regrows or when there is a significant risk that it will regrow (Meningioma II or III); when the meningioma is inoperable because of its location or the fragility of the patient because co-morbidities or his age.
The effects of radiation therapy are not immediate, but occur over time. Gradually, the tumor will stop growing and in some cases decrease in size. It disappears exceptionally.
There are two techniques for delivering radiation: a single high dose (stereotactic radiosurgery) or multiple low doses (split radiotherapy).
Radiosurgery (Gamma knife, Cyberknife, Novalis) delivers a high dose of radiation in one or a few sessions. Although there is the word surgery in radiosurgery, no incision is made. This is because the accuracy of the irradiation is similar to surgery .
For this treatment, the head must be completely immobilized either by a frame attached to the head or by a custom-made facial mask.
Fractional radiotherapy is carried out over 5 to 6 weeks with a session every day of the week with a rest at the weekend. A mask is used to accurately locate the tumor. Delivering only a small fraction of the total radiation dose each day allows normal cells to repair between treatments session. This reduces the side effects.
Surveillance
After treatment, whether surgical or radiotherapy, the patient is followed regularly and must have MRI control for many years. Although the risk of recurrence decreases over time, a recurrence can still occur a long time after treatment.
Research
- Clinical research: The data concerning the patients treated in our service are studied in order to better understand these tumors and to evaluate the results of the treatments that we propose. Our department is particularly interested in the links between meningiomas and treatments based on exogenous sex hormones (contraceptive pills, hormonal replacement therapy for menopause, hormonal treatments for gynecological pathology such as endometriosis).
- Basic research: Small fragments of all meningiomas operated in our department are stored for research purposes. The preservation of these small pieces of tumor is necessary to understand the origin of these tumors and the development of new treatments. This storage of part of the meningioma removed at the time of the intervention is done only after information and obtaining the agreement of the patient. Consent form is given to patients before each intervention. These samples are stored in the biobank of the Lariboisière Hospital within the CRB (Biological Resource Center)